DOWNLOAD
Download a PDF version of the SEMH strategy.



Download a PDF version of the SEMH strategy.
The 2020-2023 Children’s Trust Plan – refreshed from 2017-2020, has six priorities. This social, emotional and mental health (SEMH) strategy has been elevated into a stand-alone strategy, whilst retaining critical links to the other five priorities in the Children’s Trust Plan. The full six priorities are:
In addition, the Children’s Trust Plan 2020-2023 has a strategic spine – five areas that all strategies need to progress:
C. SEMH partnership, integration and I-Thrive
E. Expected outcomes and measures of success
F. COVID-19 and likely impact on emotional and mental health
G. SEMH strategy – 10 key objectives
J. Finance
Updated September 2021
There is a clear-shared intention to adopt a whole system approach to developing and transforming the support for children and young people’s mental health and wellbeing. Fundamental to this approach is the importance of partnership working and that social and emotional mental health becomes ‘everyone’s business’ in the same way as safeguarding has become ‘everyone’s business’ across Portsmouth.
We want all children and young people in Portsmouth to enjoy good emotional wellbeing and mental health. The ways in which we will achieve this vision is by:
Over the past 12-months young people, their families and the services they access have seen unprecedented challenges brought about but the coronavirus pandemic. Already increasing identification of SEMH needs have seen a steep upward trajectory, in line with nationally reported trends.
Portsmouth is a unitary authority with an estimated population 212,800 in 2020; this is forecast to increase to 218,300 by 2027 . Children in the city face significant challenges around deprivation with approximately 24% of children in the city living in poverty (the England average is 20%). However, in some areas of the city, the proportions are much higher, for example, in Charles Dickens ward, 46% of under-16s are growing up in poverty.
Portsmouth’s children and young people are predominantly of white ethnic origin (82.4%). A sizeable proportion are not of White ethic origin (i.e. 17%), with larger ethnic minorities being Bangladeshi and African.
Key findings – Children and Young People’s Needs Assessment 2018: (Estimates are based on modelled data)
In the January 2021 census there were 1,181 children and young people in reception to year 11 with EHCP’s. 228 of these pupils had a primary area of need recorded as SEMH. There were a total of 26,213 children and young people in Reception to Year 11, in state-funded Portsmouth schools.
We know locally that children with Social Emotional Mental Health needs are disproportionally represented amongst those with poor attendance and high levels of exclusion.
Data from PHE shows that across England the percentage of secondary school pupils with SEN identified as having a primary need of social, emotional or mental health (SEMH) expressed as a percentage of all school pupils in 2020 was 2.67%. This was significantly higher than in recent years. The proportion in Portsmouth is higher than the national average with 3.68%. The proportion across the South East is 2.63% with Southampton (4.05%,) and the IOW (3.42%).
Amongst the primary school age category, the recent trend has also increased with a prevalence across England of 2.45% in 2020.
Portsmouth’s proportion is 3.1% with Hampshire being 2.36%, Southampton (3.73) and IOW (3.08).
Kooth
The Kooth platform for Portsmouth launched in January 2021. Take up by young people started very well:
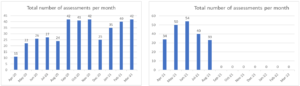
MHST referrals
The numbers of MHST referrals have been steadily rising month on month, which is expected as the teams become better established across the schools system. Of those referrals triaged 76% were accepted for assessment, we anticipate this figure will improve as schools better understand the MHST criteria and scope.
| 2021 | Jan 21 | Feb 21 | Mar 21 | Apr 21 | May-21 | Jun 21 | Jul 21 |
| Sum of Referrals | 27 | 29 | 82 | 34 | 44 | 51 | 76 |
MHST have introduced a school engagement tracker which gives a breakdown of referrals by individual schools. The tracker, which is monitored by the MHST steering group, also highlights how embedded the teams are in those schools and what they are doing to improve the partnership.
Core CAMHS – Referrals to CAMHS single point of access:
| 2018-19 | Apr-18 | May-18 | Jun-18 | Jul-18 | Aug-18 | Sep-18 | Oct-18 | Nov-18 | Dec-18 | Jan-19 | Feb-19 | Mar-19 | Total |
| Sum of Referrals | 103 | 159 | 152 | 144 | 86 | 134 | 162 | 193 | 137 | 169 | 140 | 164 | 1743 |
| 2019-20 | Apr-19 | May-19 | Jun-19 | Jul-19 | Aug-19 | Sep-19 | Oct-19 | Nov-19 | Dec-19 | Jan-20 | Feb-20 | Mar-20 | Total |
| Sum of Referrals | 122 | 150 | 153 | 151 | 82 | 118 | 165 | 149 | 112 | 140 | 133 | 92 | 1567 |
| 2020-21 | Apr-20 | May-20 | Jun-20 | Jul-20 | Aug-20 | Sep-20 | Oct-20 | Nov-20 | Dec-20 | Jan-21 | Feb-21 | Mar-21 | Total |
| Sum of Referrals | 43 | 49 | 90 | 111 | 59 | 123 | 156 | 173 | 131 | 90 | 106 | 132 | 1263 |
The CAMHS waiting lists at the start of August 2021 are:
Eating disorders
Demand for eating disorder support has started to significantly rise locally in line with regional/national trends with 33 young people in Qtr 1 2021/22 compared to 10 in Qtr 4 2021/22. The eating disorder charity BEAT reported an 81% increase in contact across all helpline channels with a 139% surge in online group attendance. Kooth report a sharp increase in eating difficulty presentations in under 18’s since the start of the pandemic.
There are currently 58 young people on the eating disorder caseload. We continue to meet the national access standards for eating disorders with 100% of urgent referrals being seen within 5 working days and 100% of routine referrals being seen within 20 working days in Qtr 1 of 2021/22.
| 2019/20 | 2020/21 | 2021/22 | ||||||||||
| Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | |
| Urgent | ||||||||||||
| Number seen within 1 week | 0 | 7 | 9 | 5 | 14 | 12 | 5 | 5 | 3 | |||
| Total Completed Cases | 0 | 9 | 9 | 5 | 14 | 12 | 6 | 6 | 3 | |||
| % Seen within Timescales | 78% | 100% | 100% | 100% | 100% | 83% | 83% | 100% | ||||
| Routine | ||||||||||||
| Number seen within 4 week | 1 | 1 | 3 | 1 | 1 | 1 | 2 | 4 | 30 | |||
| Total Completed Cases | 1 | 1 | 6 | 8 | 1 | 5 | 2 | 4 | 30 | |||
| % Seen within Timescales | 100% | 100% | 50% | 13% | 100% | 20% | 100% | 100% | 100% | |||
| Total | ||||||||||||
| Number seen within 4 week | 1 | 8 | 12 | 6 | 15 | 13 | 7 | 9 | 33 | |||
| Total Completed Cases | 1 | 10 | 15 | 13 | 15 | 17 | 8 | 10 | 33 | |||
| % Seen within Timescales | 100% | 80% | 80% | 46% | 100% | 76% | 88% | 90% | 100% | |||
Paediatric Psychiatric Liaison
CAMHS liaison continue to experience staffing pressures due to recruitment and COVID related issues, which is affecting their ability to deliver a full comprehensive service. It’s expected the service will be at full capacity in October 2021.
The No Limits service is now well established with the youth worker provision. Data in quarter 1 2021/22 highlights No Limits supported 89 young people in the emergency department.
100% of the young people who had contact with an emergency department youth worker rated the support they received as excellent or very good.
Feedback from paediatric staff has also been very positive with awareness being high (90%) and 100% of staff said the service was available when called upon.
‘We have really valued their support with patients, especially with signposting to services and linking them into resources. They’ve also been very effective at supporting patients who are distressed in the department without a parent present, as clinical staff aren’t always able to spend prolonged periods of time with each patient due to clinical demand.’
National Access Indicator
We just missed out on meeting the national access target (35%) for 2020 – 2021. Our final year rate for 2020/21 was 34.25%. The collective figure for HIOW was 40%. Work is underway to enable school nursing to flow their emotional health related work to the MHSDS. No Limits will be flowing activity as from September 2021. One of the difficulties we have locally in meeting the national access target is that the approach our CAMHS local authority offer takes; supporting the network to support the young person, a ‘team around the worker’ approach. As this work isn’t direct one to one work with the young person it doesn’t count towards the target.
Partners across Portsmouth are fully signed up to the SEMH strategy and have a very successful Portsmouth Education Partnership which brings together LA maintained schools, academy providers, the council and health partners.
Good social and emotional mental health for children and young people and closing the gap around inequalities is a key priority for Portsmouth and is a golden thread running through our strategies and plans. We have a strong track record of excellent partnership working through a long-established set of Children’s Trust arrangements. The SEMH Partnership includes:
Integration, Integration, Integration – What does it look like?
We use a relationship-based approach to promote and develop SEMH so that all children and young people can flourish in our local community. This approach recognises the importance of:
Coproduction
Partners across the Portsmouth system have set coproduction at the heart of improvement and transformation work. The Partnership aim to work in coproduction wherever possible in order to achieve the best outcomes for those who make use of our services. This includes individual, operational and strategic co-production. Representatives from Portsmouth Parent Voice, Dynamite (young people’s group) and Portsmouth Parent Board are all represented on both the Strategic partnership and sub-groups.
The coproduction strategy can be found in Appendix B.
The I-Thrive framework is being used to support system-wide change. Portsmouth is transforming its approach to children and young people’s emotional wellbeing and mental health by aligning itself with the Thrive model. The framework is an approach to supporting all children and young people’s emotional wellbeing. We know that the influences on a child mental health are varied and each and every individual in a community has a role to play in helping young people to stay emotionally healthy.
All our service and pathway developments will follow these principles.
| Principles | Description |
| Common language | Provides a shared language which everyone can understand. |
| Needs led | Approach based on meeting needs regardless of diagnosis. |
| Shared decision making | Children, young people and their families are experts in understanding their needs. |
| Proactive early intervention and prevention | Enabling the whole community in supporting mental health and wellbeing. |
| Partnership working | Working together to support and improve mental health is vital – ‘everybody’s business’. |
| Outcome informed | Shared understanding of what we are trying to achieve and understanding early if it is not working. |
| Reducing stigma | Reducing together the stigma that surrounds mental health. |
| Accessibility | Advice, help and risk support available in a timely way for the child, young person or family, where they are and in their community. |
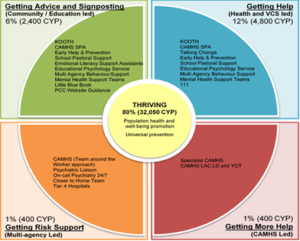
To help us as a system understand how many children and young people (CYP) have emotional health needs and the level of their need we have used the findings of the national Thrive programme to identify what the potential demand might be in each of the Thrive clusters. The authors of the Thrive elaborated report (an update on 2015 of the original Thrive paper) indicate that 80 to 90% of young people can be said to be Thriving. Of the remaining 10-20% of young people:
The population estimate indicates there are 40,050 children and young people aged 5 to 19. These weightings have been applied to the local population of young people in Portsmouth and the results are set out below.
| % | Number | |
| estimated young people thriving | 80% | 32050 |
| estimated getting advice | 6% | 2400 |
| estimated getting help | 12% | 4800 |
| estimated getting more help | 1% | 400 |
| estimated getting risk support | 1% | 400 |
| Total aged 5-19 | 100% | 40050 |
| Total not “Thriving” | 20% | 8000 |
| Population source: ONS 2018-based subnational projection for 2020 rounded to nearest 50; and percentages from Table 1 of Warrington’s THRIVE cluster report | ||
We have decided to base the modelled data on the assumption 80% of children and young people are thriving. The reason for us using this more conservative projection is that the prevalence figures this modelling is based on would be out of date with the known rising demand for children’s mental health support.
When reviewing our service data alongside the modelled data we know that there are currently large numbers of young seeking specialist support in the getting more help section as opposed to the numbers needing support in the getting advice and getting help sections. This reinforces our plans to provide greater access to self-help and early help support which in turn will prevent difficulties escalating and requiring specialist mental health services.
It’s estimated that roughly 8,000 of children and young people in Portsmouth are not thriving and would benefit from some form of social emotional mental health support. Our plan is to continue comparing this modelled data with service data which will give us a better understanding for what demand would be in each THRIVE cluster.
The SEMH Partnership have agreed a system-wide scorecard that will provide a picture of both service improvement and impact for young people. This seeks not only to measure performance where necessary, but moreover to inform the system about where positive outcomes are seen and where focus should be given to make further strides forward for young people. The scorecard groups data under 4 areas; quantity, quality, impact and feedback. This helps the system to understand whether we have sufficient resources, whether we are delivering high-quality provision that is impacting on young people’s outcomes and draws on user and provider feedback for continuous improvement.
The SEMH Strategy targets nine key outputs and outcomes, which will positively impact on young people long-term:
Measures of success based on national expectations
The SEMH partnership has considered, as a result of the COVID-19 pandemic, the likely impact and presentation of mental health difficulties within the population as a whole. We are focusing on how we reshape the system to meet an anticipated increase in demand for mental health support for children and young people as lockdown eases and children return to school and their peers.
The short-term (year one) plan in this Strategy including our response to COVID-19. ‘New’ or increased anticipated needs as a result of COVID-19 include the following:
1. Secure strong early attachment in the first 1000 days of life
| 1. Secure strong early attachment in the first 1000 days of life | |
| Named leads: Kelly Pierce | |
| Oversight: SEMH Board and Early Help Board | |
Key Achievements in last year
|
|
| Key Performance Indicators:
To be agreed |
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Remodel peri-natal mental health support |
| 2 | Improve ante-natal identification of factors leading to poor attachment |
| 3 | Review capacity of Post-Natal Depression support |
| 4 | Delivery and implementation of Under 5’s Action Plan |
| Years 2 and 3 | |
| 5 | Develop capacity within midwifery for strengthen alignment with locality Multi-Agency Teams |
2. Provide high quality advice, guidance and self-help
| 2. Provide high quality advice, guidance and self-help | |
| Named leads: Jade Simango/Stuart McDowell/Sarah Christopher/Sophie Fry | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
| Key Performance Indicators:
To be agreed |
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Coproduce a simple and accessible guide that describes the right pathway and resources to access for a range of SEMH support, how to access that support and the self-help resources both locally and nationally that help young people and families to thrive. |
| 2 | Continue to promote SEMH related support, advice and guidance as set out in the Communications Plan. |
| 3 | Public health campaign to reduce stigma and enable conversations about mental health |
| 4 | Agree a plan for how we will empower parents and carers to support their children’s wellbeing |
| Years 2 and 3 | |
| 5 | |
| 6 | |
3. Develop the children and young people’s workforce
| 3. Develop the children and young people’s workforce | |
| Named leads: Anthony Harper/Mike Bowen/Stuart McDowell | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
Key Performance Indicators:
|
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Resource and develop DDP Network – DDP Level 1 & 2 training planned in the Autumn |
| 2 | Develop a generic ‘whole workforce’ competency framework – knowledge, skills and competencies |
| 3 | Ensure capacity for continued roll-out of Restorative Practice Training |
| 4 | Ensure capacity for continued roll-out of PACE training |
| 5 | Recruit to vacant posts in CAMHS following investment |
| Years 2 and 3 | |
| 6 | Map current training offer against the competency framework |
4. Improve early help and develop digital solutions
| 4. Improve early help and develop digital solutions | |
| Named leads: Stuart McDowell | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
Key Performance Indicators:
|
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Event planned with the Children and Young Peoples Voluntary Sector Partnership |
| 2 | Continue to promote Early Help offer to the community |
| 3 | Embed the Silvercloud Evidenced Based platform in the MHST/CAMHS SPA offer |
| 4 | Refresh the Parent’s ‘Behaviour Management’ offer on the back of the SEMH Pathway review |
| Years 2 and 3 | |
| 5 | Review impact of Kooth and Silvercloud |
5. Improving wellbeing and resilience in education
| 5. Improving wellbeing and resilience in education | |
| Named leads: Sarah Christopher/Stuart McDowell | |
| Oversight: SEMH Board and SEND Board (Inclusion Group) | |
Key achievements in last year
|
|
Key Performance Indicators:
|
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Recruit the additional Behaviour Specialist and Digital Communication role in the MHST’s |
| 2 | Hold a number of MHST awareness webinars for primary/secondary heads and mental health leads |
| 3 | Continue to roll out training and support as part of the Wellbeing for Education Return (post lockdown). |
| 4 | Create clear pathways and alignment between schools, MHSTs and Early Help and Prevention |
| 5 | Promote the PIE QM to help schools to evaluate and improve their whole school mental health approach |
| Years 2 and 3 | |
| 6 | Wellbeing Peer Mentoring programme to be established |
| 7 | Increased use and understanding of supervision for staff in pastoral roles |
6. Improve mental health support for LAC and care leavers
| 6. Improve mental health support for LAC and care leavers | |
| Named leads: Danielle Tully | |
| Oversight: SEMH Board and Corporate Parenting Board | |
Key achievements in last year:
|
|
Key Performance Indicators:
|
|
| No. | Key Deliverables: 2021 – 2023 |
| Year One | |
| 1 | Review of SDQ process and embedding of SDQ in care planning |
| 2 | Review of trauma informed training programme |
| Years 2 and 3 | |
| 3 | Development of a LAC/Health Joint Working Protocol |
| 4 | Review Health Passport |
7. Improve the support for specific groups of vulnerable children and young people
| 7. Improve the support for specific groups of vulnerable children and young people | |
| Named leads: Hayden Ginns/Jade Simango/Sarah Christopher/Stuart McDowell | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
Key Performance Indicators:
|
|
| No. | Key Deliverables – 2021 – 2023 |
| Year One | |
| 1 | Agree a costed DDP training development plan including target groups of children and families and the professional network |
| 2 | Review how we address the emotional health needs of children and young people who identify as LGBTQ + |
| 3 | Identify what needs to be done to improve access to, experience of and outcomes from mental health services for Black, Asian and minority ethnic communities in Portsmouth |
| Years 2 and 3 | |
| 4 | Develop child and family support team at Harbour school (Health and Justice and OPCC funding) |
| 5 | Session planned between CAMHS and EHP’s LGBTQ Team to explore how the service could be more inclusive. |
8. Develop CAMHS services to meet demand
| 8. Develop CAMHS services to meet demand | |
| Named leads: Sonia King | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
Key Performance Indicators:
|
|
| Key Deliverables: 2021 – 2023 | |
| Year One | |
| Review the CAMHS LD offer with the ambition that this offer is available across all mainstream schools | |
| Introduce self-referral pathways for Eating Disorder support. | |
| To fully embed outcome measurements across the service in line with local and national expectations | |
| Align CAMHS Liaison and No Limits. Undertake ‘journey of child’ mapping to streamline process and clarify functions. | |
| Evaluate No Limits offer to evidence impact and inform future commissioning | |
| Years 2 and 3 | |
| Actively engage in piloting and trialling new ways of working which will inform the long-term delivery of services across the wider system | |
| Ensure pathways into and out of CAMHS are fully aligned with MHST, early help and safeguarding pathways | |
9. Prevent suicide and its impact on children, young people and families
| 9. Prevent suicide and its impact on children, young people and families | |
| Named leads: Jane Leech/Jade Simango | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
| Key Performance Indicators:
To be agreed |
|
| Key Deliverables:2021 – 2022 | |
| Year One | |
| Roll out ‘School Postvention Protocol’ that includes information and tools to support the School/College community | |
| Tender planned for the all age suicide specific bereavement service to go live in 2022 | |
| Years 2 and 3 | |
| Include targeted approach to suspected suicide real time surveillance (RTS) development to 18-25 age range | |
| Suicide real time surveillance (RTS): Engage with Safeguarding Teams to strengthen relationships around suicide prevention, suspected suicide notifications and collaboration on postvention | |
| Collaborate with Police colleagues to defining criteria for each level/tier of suspected suicide notification and anticipated response from local partners. | |
| Portsmouth Suicide Prevention Partnership pivot priority area – debt & unstable employment to specifically target work 18-25 age, parents & carers | |
10. Improving our local knowledge and performance management
| 10. Improving our local knowledge and performance management | |
| Named leads: Stuart McDowell/Hayley Webb | |
| Oversight: SEMH Board | |
Key achievements in last year:
|
|
| Key Performance Indicators:
n/a |
|
| Key Deliverables: 2021 – 2022 | |
| Year One | |
| Agree and receive a full dataset from partners, including Solent NHS Trust | |
| Fully embed Performance Scorecard Approach to all commissioned services – strengthening voice of and experience of the child and family | |
| Ensure School Nursing and No Limits are able to flow their emotional health related work to the MHSDS | |
| Years 2 and 3 | |
One of six multi-agency boards as part of the Portsmouth Children’s Trust and reporting into the Health and Wellbeing Board, governance of all commissioning and service design is through the SEMH board.
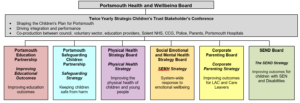
The SEMH Board meets on a quarterly basis and is chaired by Hayden Ginns, Assistant Director Commissioning and Performance, Children’s Services and Education & Portsmouth CCG. The board monitors progress through a quarterly report and the SEMH Performance Scorecard.
The SEMH Board focuses on; data and performance indicators, progress of the implementation plans, what’s going well and what needs to improve. There is an annual progress report submitted to the Health and Wellbeing Board reporting impact across all priorities.
There has been significant investment to transform the capacity and performance of the children and young people’s mental health offer in Portsmouth over the last year.
| Overall MHIS spend | 18/19 | 19/20 | 20/21 | 21/22 FOT | |
| £000 | £000 | £000 | £000 | ||
| Children & Young People’s MH (exc LD) | £ 2,291.00 | £ 2,611.00 | £ 2,691.00 | £ 2,810.00 | |
| Children & Young People’s Eating Disorders | £ 105.00 | £ 110.00 | £ 212.00 | £ 329.00 | |
| £ 2,396.00 | £ 2,721.00 | £ 2,903.00 | £ 3,139.00 | ||
| Annual increase in investment | |||||
| Children & Young People’s MH (exc LD) | £ 320.00 | £ 80.00 | £ 119.00 | ||
| Children & Young People’s Eating Disorders | £ 5.00 | £ 102.00 | £ 117.00 | ||
| £ – | £ 325.00 | £ 182.00 | £ 236.00 | ||
| National Ambitions Investment Tool – Annual increase in CCG baseline funding | |||||
| Community based services and crisis services | £ 94.61 | £ 133.08 | £ 111.31 | ||
| Eating disorder services | £ 41.67 | £ 40.73 | £ 2.04 | ||
| £ – | £ 136.28 | £ 173.81 | £ 113.35 | ||
In addition to the core spend outlined above, it is worth noting the substantial investment in Mental Health Schools Teams (MHST) in the City (circa £900,000 per annum when fully implemented) and the bespoke CAMHS contracting Portsmouth City Council has in place, spending £356,000.